Laser vs. Traditional Cataract Surgery: Which is Right for You?

If you've been told you need cataract surgery, you've probably come across two options: traditional surgery and laser-assisted surgery. Both are safe, both are effective, and both are performed right here in Brisbane — but understanding the difference helps you walk into your consultation feeling informed rather than overwhelmed. The choice between them isn't about which is "better" in general — it's about which is better for your specific eyes.
The Evolution of Eye Surgery
To appreciate how far cataract surgery has come, it helps to know where it started.
In the early days of ophthalmology, cataract surgery was a major procedure. Patients spent days in the hospital, lay still with sandbags around their heads to prevent movement, and recovered for weeks. Vision results were inconsistent, and complications were far more common than they are today. The artificial lenses we now take for granted didn't even exist until the 1950s, when British surgeon Sir Harold Ridley first implanted one — an idea that was initially met with scepticism by the medical establishment.
The introduction of phacoemulsification in the late 1960s and early 1970s changed everything. Instead of removing the entire lens through a large incision, surgeons could now break it up with ultrasound energy and remove it through a tiny opening. Hospital stays are shortened. Recovery times dropped. Results improved dramatically.
Then came the next leap: femtosecond laser technology, first applied to cataract surgery around 2008–2010. This allowed certain steps of the procedure — previously performed by hand with a blade — to be guided by a computer-controlled laser with extraordinary precision. Dr Binetter was among the first surgeons in Australia to adopt modern cataract and laser eye surgery techniques, and he has refined his approach over more than 35,000 procedures since. That history matters when someone is operating millimetres from your retina.
Today, cataract surgery is a 15-minute procedure, performed under light sedation, with most patients back to their daily routine within days. It is one of the most commonly performed and most successful surgical procedures in the world.
How Traditional Cataract Surgery Works
Traditional cataract surgery — known as phacoemulsification — remains the most widely performed cataract technique globally. It is highly refined, exceptionally safe, and produces outstanding results for the vast majority of patients. The word "traditional" can make it sound outdated, but that's misleading. A better way to think of it is proven.
Here's how it works in plain English:
Anaesthetic eye drops are applied to numb the eye completely. Most patients also receive a light sedative to help them relax.
A tiny incision (around 2–3mm) is made at the edge of the cornea — the clear dome at the front of your eye.
A circular opening is carefully created in the front of the lens capsule (the thin membrane that holds your natural lens in place). This step is called a capsulotomy.
A fine ultrasound probe is inserted through the incision. It emits rapid sound waves that break the cloudy natural lens into tiny fragments — a process called phacoemulsification.
The fragments are gently suctioned out through the same probe.
A foldable artificial lens (called an intraocular lens, or IOL) is rolled up and inserted through the tiny incision, then unfolds into position inside the capsule.
The incision is self-sealing — in most cases, no stitches are needed at all.
The entire procedure typically takes 15 minutes. You go home the same day. Most people notice a significant improvement in their vision within 24 hours, with full clarity settling over the following few weeks as the eye heals.
The safety record of phacoemulsification is outstanding. In experienced hands, serious complication rates are extremely low — around 1 in 1,000 cases or better. For most patients with a routine cataract, this is all they will ever need.
How Laser-Assisted Surgery Works
Laser-assisted cataract surgery — known as FLACS (Femtosecond Laser-Assisted Cataract Surgery) — adds a computer-guided laser step at the beginning of the procedure. Rather than replacing phacoemulsification entirely, it uses a femtosecond laser to perform some of the most delicate manual steps with a level of precision that even the most skilled hands cannot replicate consistently.
A femtosecond laser fires incredibly rapid pulses of light — each lasting one quadrillionth of a second — to separate tissue at a microscopic level without generating heat. Before surgery begins, a 3D map of your eye is captured and fed into the laser system, which then works to a plan tailored precisely to your eye's unique measurements.
Specifically, the femtosecond laser can perform:
The corneal incision — made to exact depth, length, and angle, based on your individual corneal measurements
The capsulotomy — the circular opening in the lens capsule, which the laser makes with near-perfect roundness and centration, far more consistently than is possible by hand
Pre-softening of the cataract — the laser fragments the cloudy lens into a grid pattern before the ultrasound probe is even introduced, meaning less ultrasound energy is needed inside the eye during phacoemulsification
That reduction in ultrasound energy is significant. The less energy used inside the eye, the less stress on the surrounding structures including the corneal endothelial cells that keep your cornea clear. For patients with particularly dense cataracts or those who are more vulnerable to this kind of stress, this can be a meaningful clinical advantage.
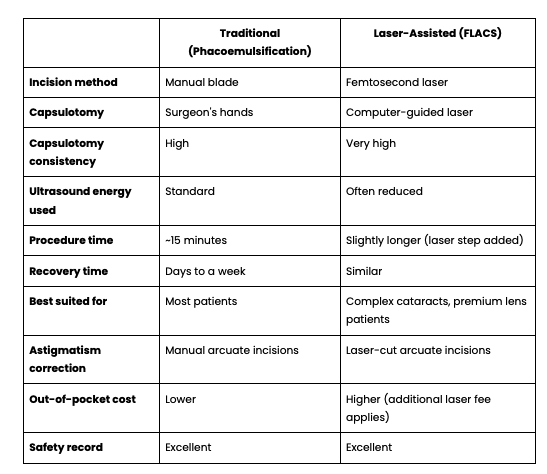
Side-by-Side: What’s the difference?
When Is Laser Worth the Extra Investment?
This is the question patients ask most often, and it deserves a straight answer.
The femtosecond laser offers the most meaningful clinical benefit in the following situations:
1. Premium or multifocal lens implants
If you're considering a premium lens — one designed to give you good distance and reading vision, reducing your dependence on glasses — the laser's precision becomes especially valuable. Multifocal lenses are sensitive to positioning. A perfectly centred, circular capsulotomy gives the lens the best possible platform to perform as designed. A slightly off-centre opening can compromise the result even when the lens itself is perfect.
2. Toric lenses for astigmatism
Toric IOLs correct astigmatism by sitting at a very specific rotational angle inside the eye. The laser's accuracy in creating the capsulotomy and the corneal incisions helps ensure the lens lands and stays exactly where it needs to be.
3. Dense or mature cataracts
When a cataract is very advanced and the lens is particularly hard, breaking it up requires more ultrasound energy. The laser's pre-softening step can reduce the energy burden significantly, which is gentler on the surrounding eye structures.
4. Patients with certain corneal conditions
Conditions such as Fuchs' corneal dystrophy make the cornea more vulnerable to stress during surgery. Reducing ultrasound energy with FLACS can help protect corneal health in these patients.
5. Patients who want maximum possible precision
For some patients, the peace of mind that comes with computer-guided laser precision has value in itself — particularly those who've been anxious about surgery, or who have high-demand vision requirements for their profession or hobbies.
For patients with straightforward cataracts, healthy corneas, and a standard monofocal lens preference, phacoemulsification in experienced hands is every bit as effective — and considerably more cost-efficient.
What About Eye Surgery Recovery?
Whether you have traditional or laser-assisted surgery, the recovery experience is broadly similar:
Day 1: Vision may be blurry or hazy — this is completely normal
Days 2–7: Most patients notice significant improvement; driving is usually possible within a week (subject to your surgeon's clearance)
Weeks 2–4: Vision continues to settle and sharpen as the eye adjusts to the new lens
6–8 weeks: Final vision is typically stable by this point
You'll be given antibiotic and anti-inflammatory eye drops to use for several weeks after surgery. Avoiding swimming, dusty environments, and rubbing your eye is important in the first few weeks. Most people find the recovery far easier than they expected.
It's also worth noting that your two eyes are operated on separately — usually one to four weeks apart — so you always have one functioning eye during recovery.
Why the Consultation Is Everything
There is no universally "right" answer between these two techniques. The correct choice depends on:
The density and position of your cataract
The shape and health of your cornea
Your prescription and whether astigmatism is a factor
The type of lens implant you're considering
Your vision goals — whether you want to be glasses-free, or are happy to use glasses for some tasks
Your overall eye health and any other conditions present
Dr. Binetter takes time at every consultation to map your eye anatomy thoroughly before making any recommendation. He uses both techniques and has no financial incentive to push one over the other — his recommendation is driven entirely by what gives you the best outcome. With over 35,000 procedures performed, he has encountered virtually every variation the human eye presents, from the most routine to the most complex.
That depth of experience is ultimately what you're investing in — not just the technology used on the day.
Take the First Step
The only way to know which approach is right for your eyes is to have them properly assessed by a surgeon who is equally skilled in both.
📞 Book your consultation at Springwood Eye Clinic today.
We'll give you a clear, honest recommendation and a full breakdown of costs before you make any decisions.